
Medieval Dunstable© Webmaster Helen Mortimer Privacy Policy | Terms of Use



Bone Study
An Osteological Study of the Dominican Friary at Dunstable
The Dominican Friary at Dunstable was founded in 1259 and dissolved in 1539. Its buildings lie to the south of the High Street in Dunstable. Since the 1830s excavations and observations of ground disturbance have taken place on the site, and before 1970 parts of buildings had been located along with burials. In the 1970s extensive work located the church, identified a boundary wall and ditch to the north of the church which could represent the precinct boundary, and confirmed the existence of what appears to be an elaborate monastic garden. In 1988 and 1990 excavations by the Bedfordshire County Archaeology Service, now Albion Archaeology, revealed 70 inhumations from the area in and around the church and an additional 10 boxes of residual bone or bone recovered from sieving. Luton Culture currently possesses all skeletal material recovered by Albion Archaeology and several other boxes of skeletal material that appear to be from the medieval cemetery but were excavated earlier. As part of a three-month post-doc project from the University of Cambridge the entire medieval friary skeletal assemblage possessed by Luton Culture received an initial assessment by the author of this article.
The Dunstable Friary collection is a very interesting assemblage, which shows high rates of disease and illness, but also that the people who were buried in the cemetery frequently lived long lives and were well cared for. In fact, the data suggests that obesity was a frequent problem of the deceased and that the cemetery likely contained not only Dominican friars, but ordinary people of respectable social status.
With regards to the skeletal data discussed above, only seventy inhumations with clear context will be examined in detail and of these, it is now speculated that at least two of the inhumations are part of other graves and so only 68 individuals will be discussed. A majority of the remaining skeletal remains are of such a mixed context it is difficult to determine true numbers of individuals and they will be discussed in a later article. The data from the Friary will frequently be compared with skeletal information on thousands of medieval individuals summarised in Roberts and Cox’s book Health & Disease in Britain (2003) which will be abbreviated as R&C’s study. Furthermore, due to the shortness of the project much of this data is only preliminary and many more studies are needed including the estimated height of the deceased. Finally, with regards to evaluating pathology rates, the osteological paradox must always be considered. The osteological paradox is that older individuals frequently show more evidence of pathologies than younger people because they survived them, and many pathologies do not lead directly to death. This point will become very clear for the Friary skeletal sample.
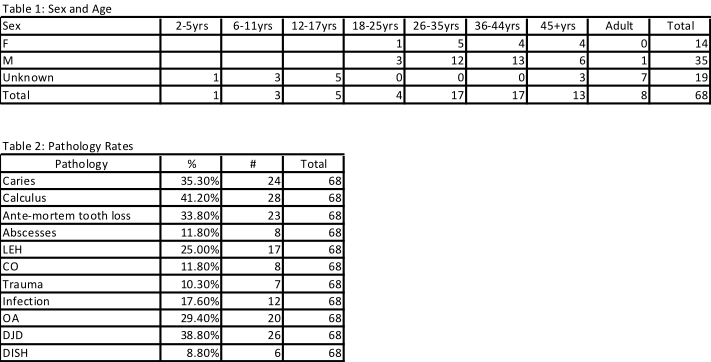
In the case of sex and age, as seen from Table 1 the Dunstable Friary cemetery possessed not only men, but women and children: 9 children, 14 females, 35 males and 10 adults of unknown sex. A large percentage of the population (19.1% – 13/68) lived to the relatively old age for the period of 45+yrs, and many of these individuals likely died in their 60s or older. Interestingly, an almost equal numbers of males and females lived to 45+yrs and this together with other data, might suggest wealthy female patrons to the Friary were buried in the cemetery.
For nutritional deficiency pathologies (Table 2) prevalence was fairly low with only 25% (17/68) having suffered from linear enamel hypoplasia (LEH) and only 11.8% (8/68) having had cribra orbitalia (CO). In comparison, for R&C’s study the rates were 35.8% and 10.3%. Both pathologies may be caused by systemic metabolic stress (malnutrition, infectious diseases and/or parasitic infection), hereditary anomalies and localised trauma and for just CO the failure to properly wean a baby to solid food. For the Dunstable population, the low frequency of both pathologies might be due to the relative old age of people from the sample and their possible high status. Cribra orbitalia, which results in pitting in the eye sockets, may disappear over time as people who have received better nutrition will heal from it. While linear enamel hypoplasia (deficiencies in enamel thickness in teeth) only occur as the teeth are forming, they can disappear as increased tooth wear destroys the surface they res. Overall, the relatively low prevalence of both, especially CO, suggests that poor nutrition was not a problem for the deceased of the Friary’s cemetery.
In the case of dental pathologies, the order of prevalence was calculus (plague) 41% (28/68), caries (cavities) 35.2% (24/68), ante-mortem tooth loss (ATML) 33.8% (23/68) and abscesses 11.8% (8/68). These rates were anticipated as calculus is simply the accumulation of plaque and it can also be confused with chalk, which was the main substance in which the burials were buried. The high rate of ATML is reflective of the old age of population and abscesses (inflammations, bone swellings below the teeth) the most severe of dental pathologies are typically the least common . Caries (cavities), characterised by pits and caused by the consumption of carbohydrates, are a common pathology in agricultural based populations. In comparison, for R&C’s study the rates were calculus 59.1%, caries 52.4%, ATML 36.4% and abscesses 26.2%. Consequently, the Friary data might also suggest that some dental hygiene was practised or access to proper treatments was available to the population.
Trauma and infection rates, meanwhile, were surprisingly high and there was a clear link between them. Trauma was found in at least 10.3% (7/68) and included several individuals who must be well cared. For example, for burial 24, the lower leg was severely broken, the fibula is very twisted and the tibia was also affected and yet the associated foot and leg bones show no evidence of the arthritis which would have be expected in having to use the leg for walking. The person clearly had assistance in getting around. The most common bones for trauma were the ribs (4 individuals) and three individuals had evidence of trauma in the form of lesions suggestive of soft trauma (non-breaks of bone). The location of traumatic injuries included the ribs, femurs, lower leg and arm bones, and several individuals had multiple trauma. There also appears to close relationship with infection as 4/7 showed evidence on infection and some of the soft tissue lesions may possibly be due to infection instead.
Infection was found in 17.6% (12/68) of the individuals and was most commonly associated with the lower legs – in 8 individuals in the form of periostitis (bone being gradually destroyed and diagnosed by pitting and irregularity of the bone surface and new bone formation) (Roberts and Manchester 2010). Other affected areas were the ribs (3), femurs (1), feet (2), spine (1), arms (1) and in one case also included sternum, clavicles and scapulae. In fact, Burial 11.88 (a 45yrs+ male) may have suffered tuberculosis and had infection on the ribs and a collapse in the spine. Burial 10.88 (a 36-44yrs male) and Burial 6.88 (a 36-44yrs female) also experienced severe infection of likely diagnostically identifiable types and further study is needed to understand the precise types of infection and disease which affected the Friary collection. While these high rates may seem to reflect badly on the status and care of the Friary population in some ways they indicate the reverse. In order for infection to leave evidence on bone it must be long standing, and consequently the afflicted people were so well cared for that either the infections took a considerable time to kill them or the people were able to survive the infections but evidence remained as with the 45+year old with infection.
As expected with a high percentage of older individuals, arthritic conditions were especially common. Osteoarthritis (OA) diagnosed by marginal osteophytes and/or new bone on a synovial joint surface (lipping), pitting on the joint surface or alteration in the bony contour of the joint (eburnation) was associated with 29.4% (20/68) of individuals. The most commonly afflicted joints were the cervical and thoracic vertebrae (11 individuals each), the shoulders (8 individuals) and lumbar vertebrae (6 individuals). Degenerative joint disease (DJD), a milder version of OA diagnosed by either lipping or porosity on a joint, was found for 36.8% (25/68) of individuals; not counting those with OA. DJD was most frequently located on the thoracic (16 individuals) and lumbar vertebrae (13 individuals) and the shoulders (5 individuals). Surprisingly, DJD was associated with less variety of joints than OA, and many cases of DJD may not reflect injury or activity but aging, as natural aging causes mild bone lipping on the vertebrae. OA and DJD were certainly associated with old age as 10/13 of 45yrs+ had OA and 6/13 had DJD. With regards to R&C’s study, 27.9% had spinal OA, 20.9% spinal DJD, 16.78% nonspinal OA, and 13.6% had nonspinal DJD.
Importantly Dunstable Friary yielded 6 cases of DISH (diffuse idiopathic hyperostosis) (10% of the 60 individuals with vertebrae) and one possible case of gout. Both of these pathologies are associated with obesity. DISH is often recognised by excessive bone lipping on the right side of thoracic vertebrae which joins at least two of them with a candle waxlike appearance and ossification of extra-spinal entheses (where muscles & tendons attach) and ligaments. It has long been associated with being caused by obesity and increased age and is probably a multisystem hormonal disorder and is much more frequently found in males. Gout, caused by deposits of uric acid, meanwhile, is diagnosed by lesions distributed asymmetrically which have a punched out appearance with overhanging edges. Seventy-five percent of cases involve the first metatarsophalangeal joint (big toe) and common sites include feet, ankle, hands, wrist and knees. All of this data correlates well with the historical literature and additional archaeological information on monastic sites. Religious sites have often been suspected of being places where men were often obese either due to corruption and access to fatty food and/or their lifestyle which may have been not physically vigorous. For, example in archaeological samples of monastic sites from the London area, DISH is found in an average of 17.2% of the populations.
Overall, this initial study of the population of the Dunstable Friary appears to show that the cemetery contained a population of not only Dominican friars, but also members of the lay community, many of whom may have been socially well off. People received proper nutrition and healthcare in life to the point that obesity was a problem for some of them. Moreover, although not discussed, few individuals showed evidence of being very muscular and the severe cases of arthritis were typically associated with those who had achieved old age. Finally, the Dunstable Dominican Friary population has much research potential and with available samples of Roman Dunstable (131 individuals- dating the 3rd-5th centuries AD) found almost adjacent to the site, and the Anglo-Saxon site at Marina Drive (49 individuals- dating to 7th century AD) located less than a mile from the Friary, it may enable us to understand health in Dunstable from AD 60 to 1539.
REFERENCES
Albion Archaeology, 1990. Excavation and Skeletal notes for Dunstable Friary. Unpublished notes. Bedford.
Alt, K., J. C. Turp & J. Wachter, 1998. Periapical Lesions-Clinical and Anthropological Aspects, in Dental anthropology: fundamentals, limits, and prospects, eds. K. W. Alt, F. W. Rösing & M. Teschler-Nicola, Wien: Springer, 247-76.
Bridges, P. S., 1992. Prehistoric Arthritis in the Americas. Annual Review of Anthropology, 21, 67-91.
Clark, R., and A. Maull, Dunstable Friary Excavations 1988. Manshead Journal 29, 26-29
Central Bedfordshire Council, 2013. Dominican Friary, Dunstable Historic Environment Record, [electronic resource] Chicksands.
Cohen, M. N., J. W. Wood & G. R. Milner, 1994. The Osteological Paradox Reconsidered. Current Anthropology, 35(5), 629-37.
Duray, S. M., 1996. Dental indicators of stress and reduced age at death in prehistoric Native Americans. American Journal of Physical Anthropology, 99, 275-86.
English Heritage, 2013. National Monuments Record, Dunstable Friary [electronic resource].
Facchini, F., E. Rastelli & P. Brasili, 2004. Cribra Orbitalia and cribra cranii in Roman Skeletal Remains from the Ravenna Area and Rimini (I-IV Centuries AD). International Journal of Osteoarchaeology, 14, 126-36.
Gardner, R., 2004. Archaeological Investigations at 24 Friary Fields, Dunstable, Bedfordshire. Bedfordshire Archaeology 25, 159-89.
Hillson, S., 2001. Recording dental caries in archaeological human remains. International Journal of Osteoarchaeology, 11(4), 249-89.
Lieverse, A. R., 1999. Diet and the aetiology of dental calculus. International Journal of Osteoarchaeology, 9(4), 219-32.
Matthews, C. L., 1962. The Anglo-Saxon Cemetery at Marina Drive, Dunstable Bedfordshire Archaeological Journal 1, 25-57.
Matthews, C. L., 1981. A Romano-British Inhumation Cemetery at Dunstable. Bedfordshire Archaeological Journal, 15.
Patrick, P.A., 2005. ‘Greed, gluttony and intemperance’? testing the stereotype of the ‘obese’ medieval monk, PhD thesis: University College London, London.
Roberts, C. & K. Manchester, 2010. The Archaeology of Disease, Stroud: The History Press.
Roberts, C. & M. Cox, 2003. Health & Disease in Britain: from prehistory to the present day, Stroud: Sutton.
Rogers, J. & T. Waldron, 2001. DISH and the Monastic Way of Life International Journal of Osteoarchaeology 11, 357-365.
Rogers, J. & T. Waldron, 1995. A Field Guide to Joint Disease in Archaeology, Chichester: John Wiley & Sons.
Sullivan, A., 2005. Prevalence and etiology of acquired anemia in Medieval York, England. American Journal of Physical Anthropology, 128, 252-72.
| Archaeology |
| Audio Guides |
| Education |
| Exhibitions |
| Events 2013 |
| Physic Garden |
| Priory History |
| Priory Churches / Lands |
| Town History |
| Virtual Tour |
| Website |
| Archaeology |
| Charters & Bylaws |
| Eleanor Cross |
| Famous People |
| The Fraternity |
| Friary |
| Guided Tours |
| History |
| Inns |
| Dunstable Treasures |
| Kingsbury |
| Middle Row |
| Royal Visits |
| Sheep & Wool Trade |
| The Town |
| Friary Archaeology |
| Bone Study |
| Friary |
| Annals Charters Valor Ecc |
| Archaeology |
| Churches and Lands |
| Guided Visits |
| Audio Guides |
| History |
| Monastic Life |
| Virtual Tour |
| The Augustinian Priory |
| The Canons Route |
| Bedfordshire |
| Buckingham |
| Derbyshire |
| Nothamptonshire |
| Hertfordshire |
| Leicestershire |
| Oxon |
| Priors |
| Annulment |
| History |
| Archives |
| Book Sales & Shop |
| Exhibitions |
| Guided Walks |
| Heritage Talks |
| Physic Gardens |
| Schools |
| Tourist Information Centre |
| Tea-room |
| Visits |
| Priory House Heritage Centre |
| Education |
| Knight |
| Search Results |